 PDF(16896 KB)
PDF(16896 KB)

Analysis of Factors Affecting Parachute Landing Injuries Based on Finite Element Modeling
RENHailong, CAOShuanghui, PENGHan, DOUQingbo, SUOTao
PDF(16896 KB)

Sponsored by: China Association for Science and Technology (CAST)
Editor-In-Chief: Xu Yida
ISSN 1000-1093
Hosted By: China Ordnance Society
Published By: Acta Armamentarii
CN 11-2176/TJ
PDF(16896 KB)
Analysis of Factors Affecting Parachute Landing Injuries Based on Finite Element Modeling
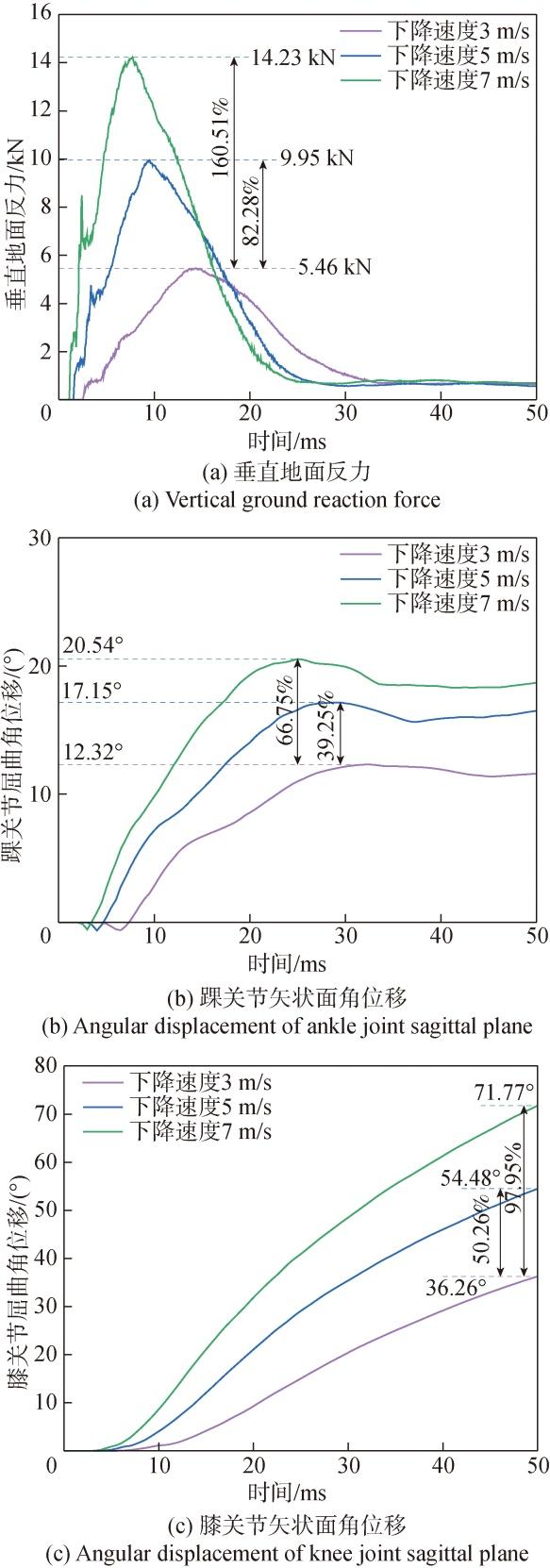
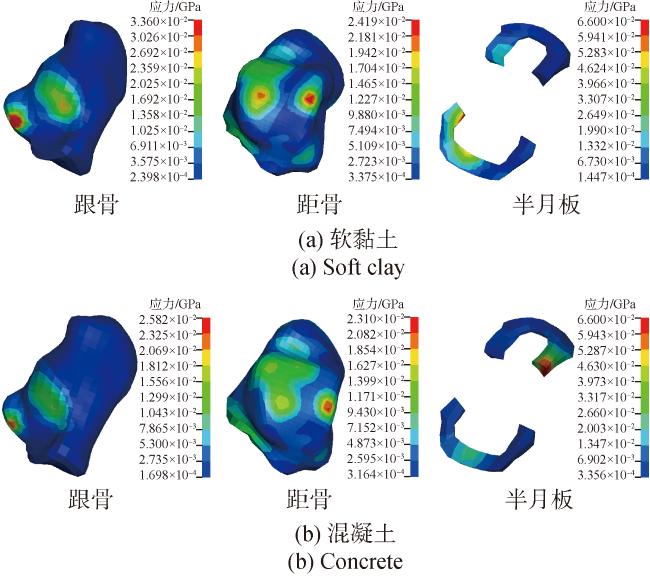
The parachute landing injuries of paratroopers have been a focal point in aviation medicine and special medical studies.It is very important to investigate the biomechanical mechanisms of landing injuries for the protection and prevention of parachute landing injuries.The factors influencing the lower limb injuries of paratroopers subjected to landing impact are numerically simulated by using the global human body models consortium (GHBMC) full-body finite element model.The findings indicate that the long bones of the lower limbs such as femur and tibia are less likely to be injured during normal landing impact.However,the calcaneus,talus and meniscus are susceptible to injury due to compression from the long bones,and the vulnerable area includes the medial tubercle of calcaneus,the trochlea of talus,and the anterior horn of lateral meniscus.The study also reveals the variations in injury mechanisms in different landing scenarios.The descent speed significantly affects ground impact forces,thereby greatly increasing the probability of stress fractures in the long bones of lower limbs.The horizontal wind speed can alter the center of gravity to increase the likelihood of ankle injuries.The ground conditions influence the duration of impact contact,increasing the probability of injuries to the ankle,particularly the calcaneus.
paratrooper / parachuting / landing injury / biomechanical mechanism / lower limb injury {{custom_keyword}} /

Table 1 General information of subjects表1 受试者基本情况 |
| 志愿者编号 | 年龄/岁 | 身高/cm | 体重/kg | 有无伤病史 |
|---|---|---|---|---|
| 1 | 22 | 176 | 72.6 | 无 |
| 2 | 23 | 173 | 74.2 | 无 |
| 3 | 22 | 177 | 75.3 | 无 |
Table 2 Comparison of platform landing experiemnts and simulations表2 平台着陆实验与仿真对比 |
| 时间/ms | 实验结果 | 仿真结果 |
|---|---|---|
| 0 |  |  |
| 40 |  | 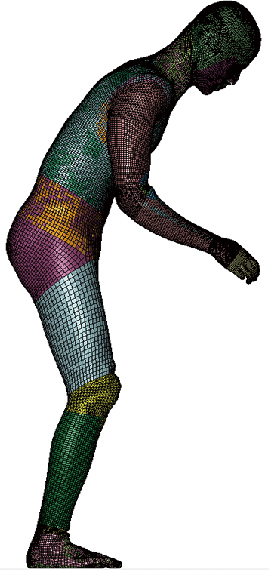 |
| 80 |  | 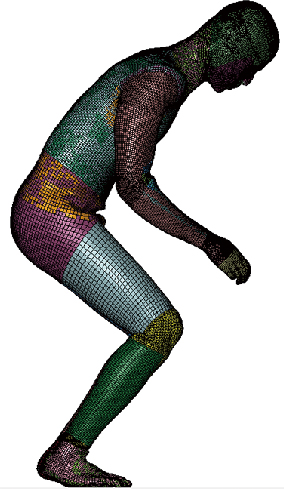 |
| 120 |  | 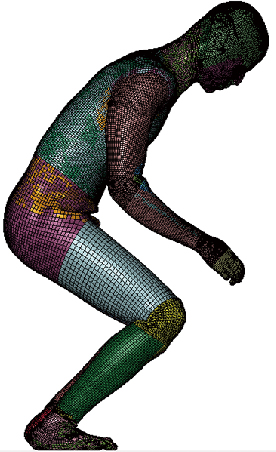 |
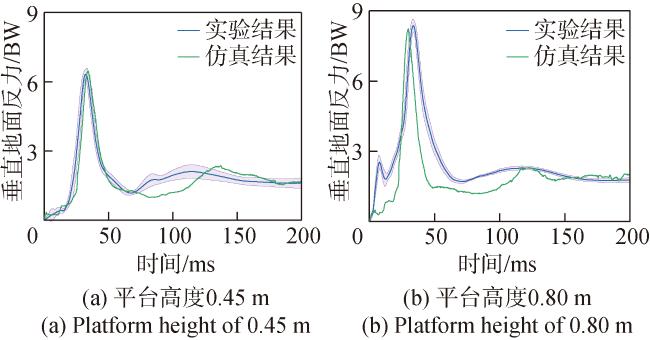
Fig.5 Comparison of experimental and simulated GRFs at different platform heights图5 实验和仿真垂直地面反力对比 |
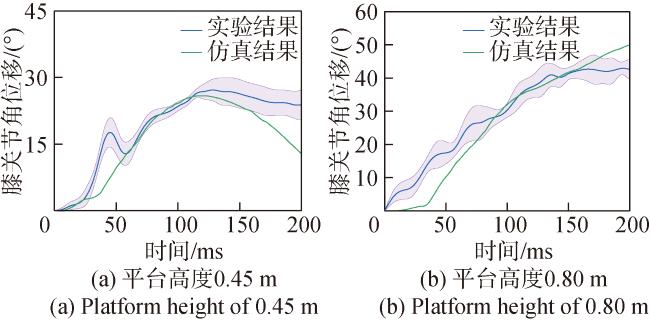
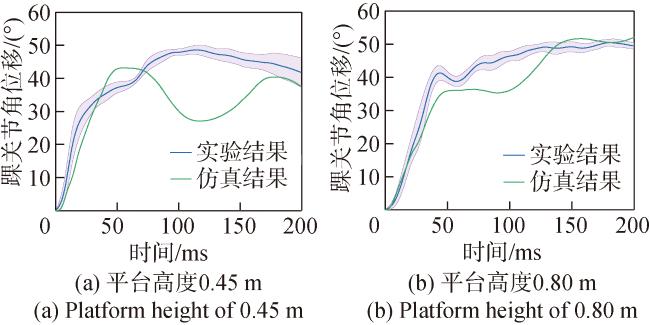
Fig.6 Comparison of experimental and simulated knee joint motion angles at different platform heights图6 实验和仿真膝关节运动角度对比 |
Table 3 Simulation parameter settings for analysis of descent speed effect表3 下降速度影响分析仿真工况参数设置 |
| 下降速度/ (m·s-1) | 水平风速/ (m·s-1) | 着陆地面 | 地面密度/ (kg·m-3) | 地面模量/ GPa | 地面 泊松比 |
|---|---|---|---|---|---|
| 3 | 0 | 混凝土 | 2500 | 30 | 0.3 |
| 5 | 0 | 混凝土 | 2500 | 30 | 0.3 |
| 7 | 0 | 混凝土 | 2500 | 30 | 0.3 |
Table 4 Simulation parameter settings for analysis of horizontal wind speed effect表4 水平风速影响分析仿真工况参数设置 |
| 下降速度/ (m·s-1) | 水平风速/ (m·s-1) | 着陆地面 | 地面密度/ (kg·m-3) | 地面模量/ GPa | 地面 泊松比 |
|---|---|---|---|---|---|
| 6 | 4 | 混凝土 | 2500 | 30 | 0.3 |
| 6 | 2 | 混凝土 | 2500 | 30 | 0.3 |
| 6 | 0 | 混凝土 | 2500 | 30 | 0.3 |
Table 5 Simulation parameter settings for analysis of ground condition effect表5 地面条件影响分析仿真工况参数设置 |
| 下降速度/ (m·s-1) | 水平风速/ (m·s-1) | 着陆地面 | 地面密度/ (kg·m-3) | 地面模量/ GPa | 地面 泊松比 |
|---|---|---|---|---|---|
| 6 | 0 | 软黏土 | 1600 | 0.01 | 0.4 |
| 6 | 0 | 粉砂岩 | 2160 | 0.2 | 0.3 |
| 6 | 0 | 混凝土 | 2500 | 30 | 0.3 |
Table 6 Injury criteria for lower limb表6 下肢损伤评价准则 |
| 下肢损伤准则 | 损伤评价指标 | 损伤阈 值/kN | 损伤概率 (简明损伤定级 标准2+) |
|---|---|---|---|
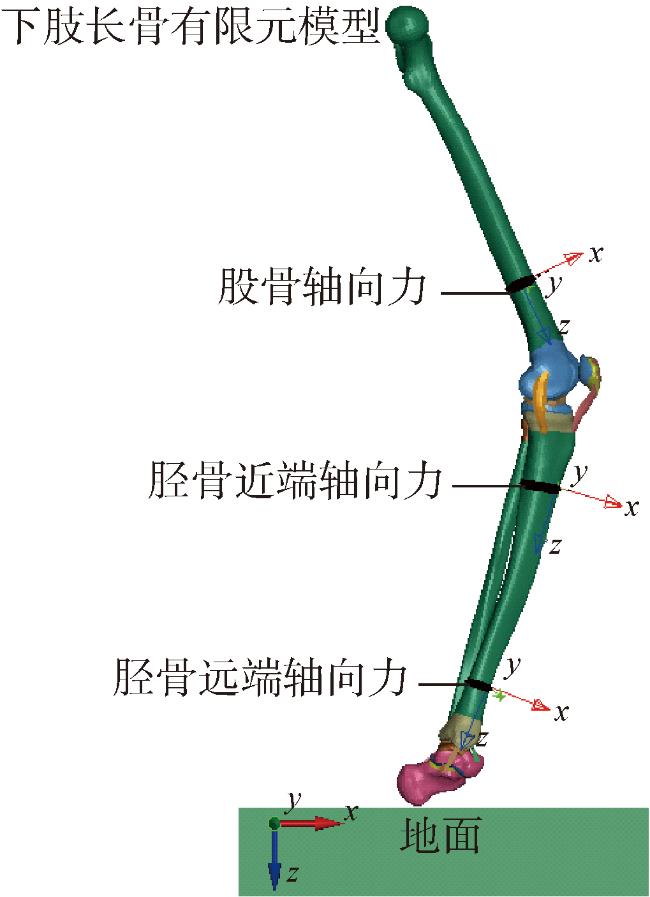
| 股骨力准则 | 股骨轴向力 | 10.00 | |
| 胫骨压缩力准则 | 胫骨近端轴向力 | 8.00 | |
| 足踝损伤准则 | 胫骨远端轴向力 | 7.59 |
| [1] |
姚文杰, 陈龙. 国外空降兵现状及发展趋势对我空降兵装备体系建设的启示[J]. 兵工学报, 2010, 31(增刊2):176-178.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [2] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [3] |
赵刚, 孙磊. 军事跳伞训练伤的发病机制影响因素及其预防[J]. 实用医药杂志, 2016, 33(2):105-108.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [4] |
曾佳敏, 仲欢, 李海波, 等. 空降兵某部义务兵和军士军事训练伤特征比较分析[J]. 军事医学, 2022, 46(6):406-409.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [5] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [6] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [7] |
While parachute jumping, soldiers may suffer minor or life-threatening injuries in various parts of the body. Several trauma scoring systems assess the severity of such injuries. The primary goal of this study was to assess clinical characteristics and the severity of orthopaedic, musculoskeletal, and other injuries from military training-related parachute jumping using two trauma scoring systems (AIS and ISS). Our secondary goal was to assess whether there was an increase in injury rates with age.In total, 185 military personnel between 19 and 51 years old who were injured as a result of daytime static parachute jumping during 44 months between January 2016 and August 2019 were included in the study. Demographic data; vital signs; the level of consciousness; the Glasgow Coma Scale; ISS trauma region classifications; anatomical injury sites; AIS and ISS scores; diagnoses; treatment methods; hospitalization status; and duration of hospital stay were examined descriptively.There were 184 male and one female participant. The most commonly injured body site was the foot (33.5%), and the most common diagnosis was soft tissue trauma (64.3%). The most commonly injured body site was the foot (33.5%), and the most common diagnosis was soft tissue trauma (64.3%). Regarding treatment methods, 51.4% received analgesic pills and cold pack application, 42.7% received a plaster splint, and 5.9% had orthopaedic surgery. The mean ISS score was 5.16 ± 3.92. The hospitalization rate was significantly higher for patients with a critical AIS score than those with a severe AIS score (p < 0.001).The use of trauma scoring systems to assess injury severity among patients admitted to an ED due to a parachute jumping injury may facilitate treatment selection. We found that AIS and ISS were useful in determining injury severity. Therefore, we recommend the use of trauma scoring systems for assessing the injury severity and the therapeutic approach, and we advocate for the use of the 17 anatomical regions we used in this study. We also found that with increasing age, the severity of injury could increase.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [8] |
This paper analyses the rate and patterns of parachuting injuries at the Sultans Oman Parachute Unit (SOPRA) in Oman.Data on 150 patients referred to Rustaq Regional Referral Hospital was collected and analysed. The injuries were defined as severe (fractures, dislocation, head trauma) or minor (contusion, bruises, sprains).The rate of severe injuries was 9 % and ankle fractures were the commonest. The minor injury rate was 13.5%. The injury rate increased in relation to age (p < 0.001). The type and possible mechanisms of injury are discussed with the recommendation for reducing the injury rates.We conclude that our data compares favourably with other studies except for higher incidence of severe injuries.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [9] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [10] |
王丽珍, 樊瑜波. 过载性损伤与防护生物力学[J]. 力学进展, 2020, 50(1):124-168.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [11] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [12] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [13] |
林鹏江, 黄峰, 叶巧, 等. 我军空降兵跳伞训练伤荟萃分析[J]. 空军医学杂志, 2020, 36(4):291-293,300.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [14] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [15] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [16] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [17] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [18] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [19] |
向福荣, 唐圣鑫, 刘鑫鑫, 等. 女性全身关节过度活动患者跳深着陆时膝关节应力分析[J]. 医用生物力学, 2023, 38(2):317-323.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [20] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [21] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [22] |
This study aimed to the biomechanics of the foot-ankle-shank complex with different boots collar heights in parachuting landing on inversion ground surface. A finite element model including tibia, fibula, ankle, foot and parachuting boot was developed. Three collar heights (low, medium, high) of the parachuting boot were simulated. Von-Mises stress, ankle inversion angle, ligament force and bone displacement were analyzed. Compared with that of the high and low collar heights, boots with medium collar height produced the lowest peak stress on the tibia and the articular cartilage of the subtalar joint. In addition, the medium collar height can better control the ankle inversion and minimize the tensile forces on the lateral ankle ligaments.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [23] |
常利军, 陈秦伟, 王天昊, 等. 弹体冲击载荷下头部损伤与防护研究进展[J]. 兵器装备工程学报, 2024, 45(7):208-216.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [24] |
范鑫, 黄星源, 常利军, 等. 枪弹冲击下头-颈动力学响应及颈部被动肌影响[J]. 兵工学报, 2022, 43(9):2200-2209.
To address the threat of projectiles and fragments in a battlefield, head-neck dynamic response to bullet impact and the effects of passive neck muscles are studied. By establishing an effective helmet-head-neck finite element model, the impact of 9 mm handgun bullets is simulated to examine the human head-neck mechanical response with or without passive muscles. The results show that in the case of front impact, stress is concentrated on the frontal head bone and the lower cervical vertebrae when the neck is extended. When the front side of the intervertebral disc fails to stretch, the passive muscles on the neck relieve the extension of the head and neck, reducing the cervical spine injury. Under the effect of passive muscles, the displacement of the head's centroid is reduced by 31.38%, and the stress exerted on the junction between cervical vertebrae and intervertebral disc as well as the maximum intervertebral disc stress are relieved by 28.76%. Thus, passive muscles play an important role in protecting the body, and thus must be considered when assessing neck injuries. The results provide reference for the assessment of neck injuries and the design of neck protective equipment.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [25] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [26] |
戴俊超, 周云波, 张进成, 等. 载人空投着陆冲击下不同乘员姿态的损伤影响[J]. 爆炸与冲击, 2021, 41(1):125-137.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [27] |
The objective of this study was to define the casualty rates and anatomical distribution of injuries associated with military static line parachute (MSLP) descents conducted by an Australian Army Commando Battalion. This study was conducted to identify the strategies to reduce the injury burden related to MSLP activities.A retrospective audit of injuries resulting from MSLP descents conducted by 4th Battalion Royal Australian Regiment (4 RAR) over a 13-month period.A total of 554 MSLP descents over the time period were reviewed. The overall casualty rate was 5.1%. For MSLP descents onto land drop zones, the incidence of injury requiring hospital admission was 2.6%. Paratrooper bodyweight was associated with increased risk of injury (P = 0.04) and hospital admission (P = 0.003), particularly when conducting descents onto land drop zones. MSLP descents conducted onto land were associated with a higher incidence of casualties when compared with those conducted into water drop zones (P = 0.001).During the period from February 2004 until February 2005, 4 RAR (Commando) experienced higher casualty rates during MSLP descents than expected when compared with the published report. Strategies to decrease the casualty rate of MSLP descents onto land drop zones may include more extensive ground training, increased frequency of MSLP descents, use of ankle braces and the development of purpose built drop zones. Consideration should be given to establishing a maximum bodyweight threshold for the conduct of MSLP activities or acquiring parachutes with decreased descent velocity for larger paratroopers.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [28] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [29] |
杨旭. 军用越野车车体在空投着陆过程的有限元分析[D]. 沈阳: 东北大学, 2021.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [30] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [31] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [32] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [33] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| {{custom_ref.label}} |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
PDF(16896 KB)
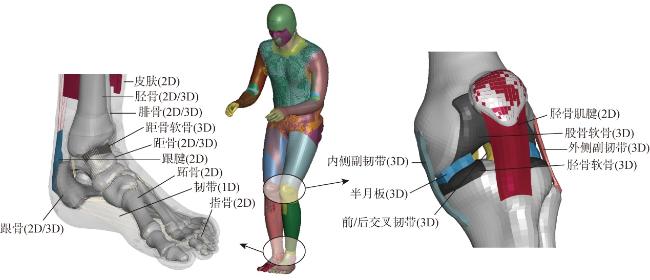
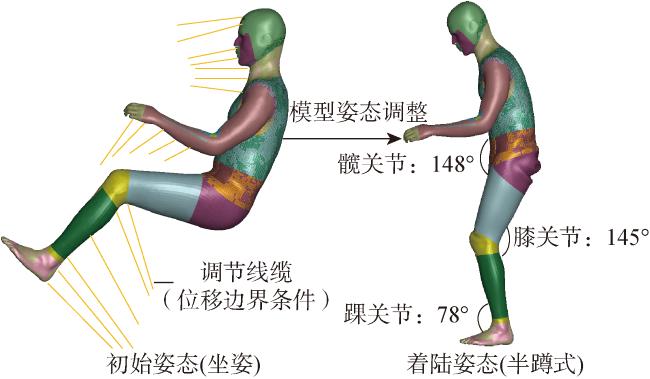
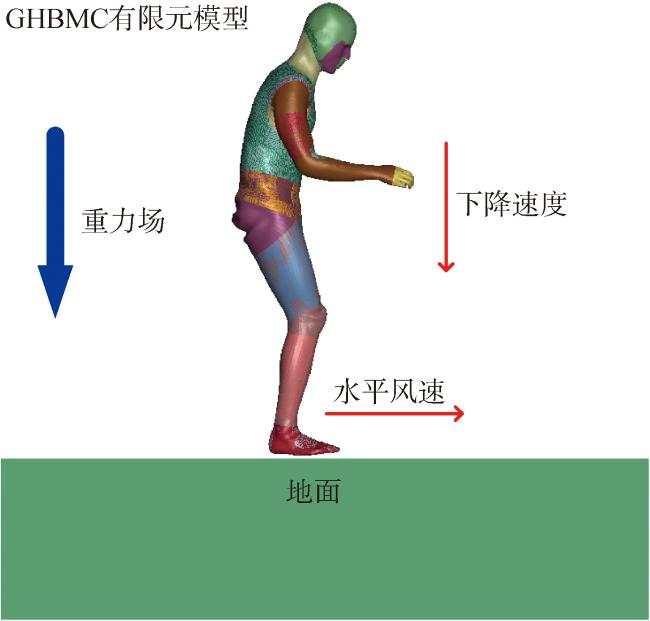
 Fig.1 GHBMC full-body finite element modelFig.2 Posture adjustment of human finite element modelFig.3 Human landing impact finite element model
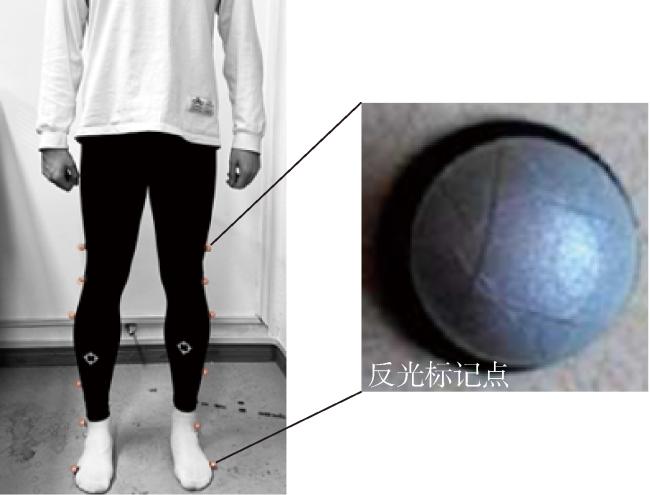
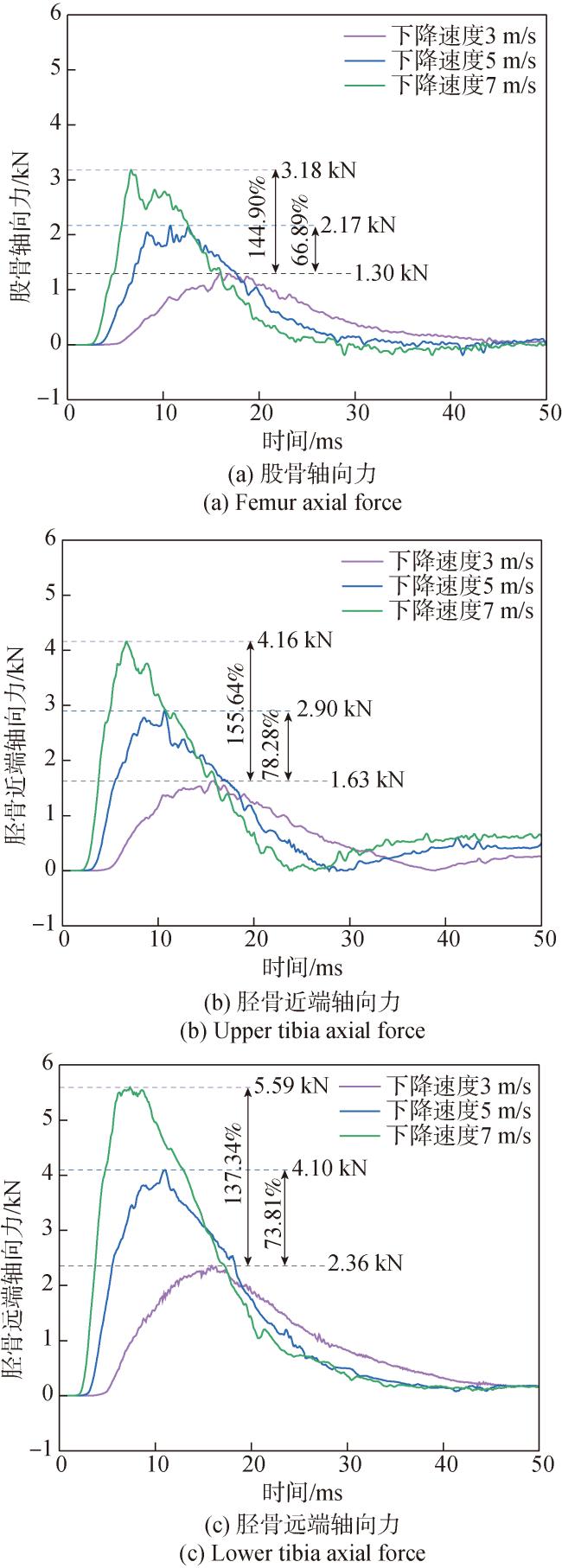
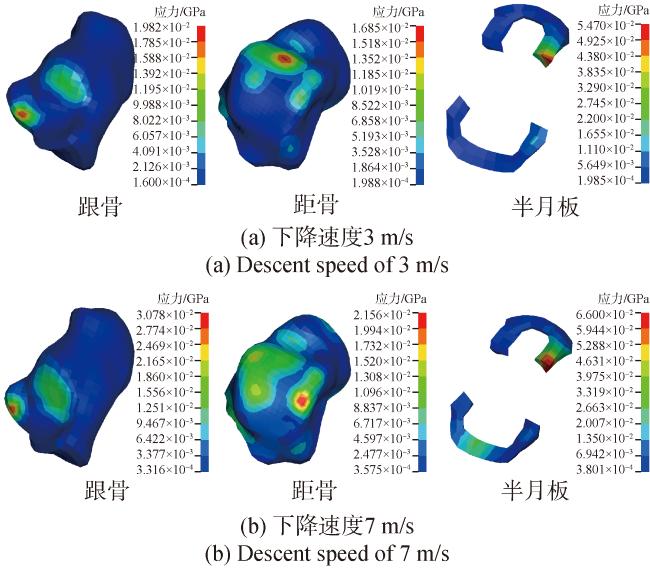
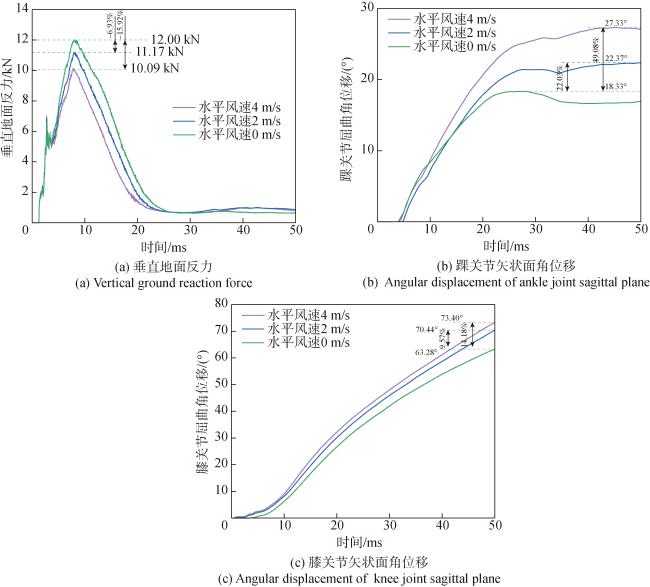
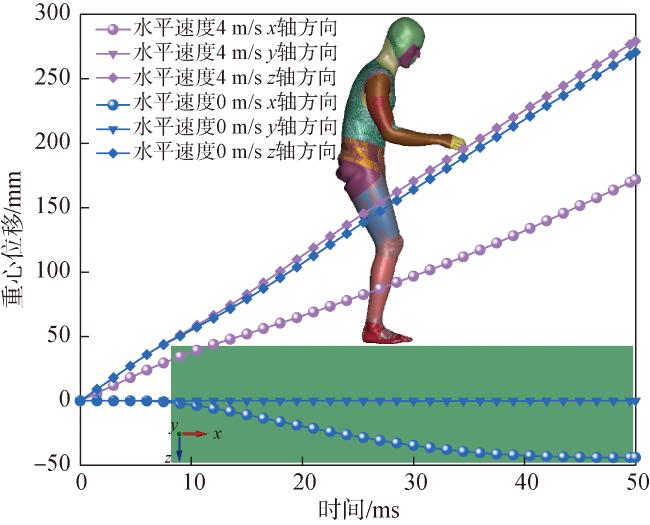
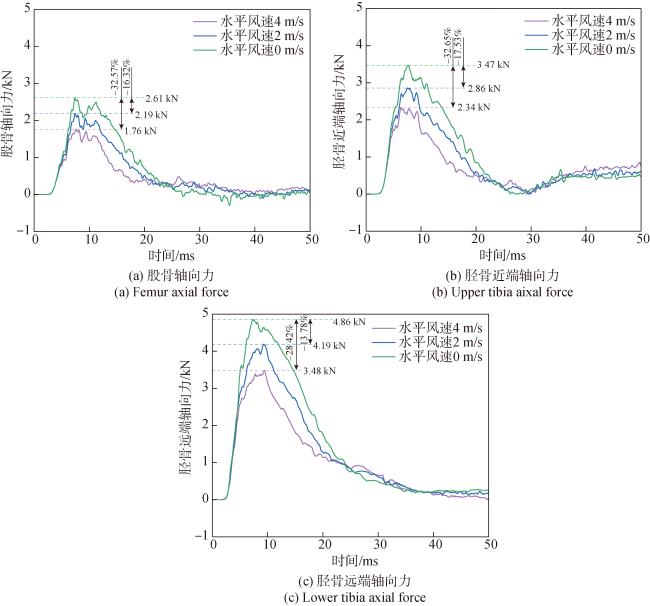
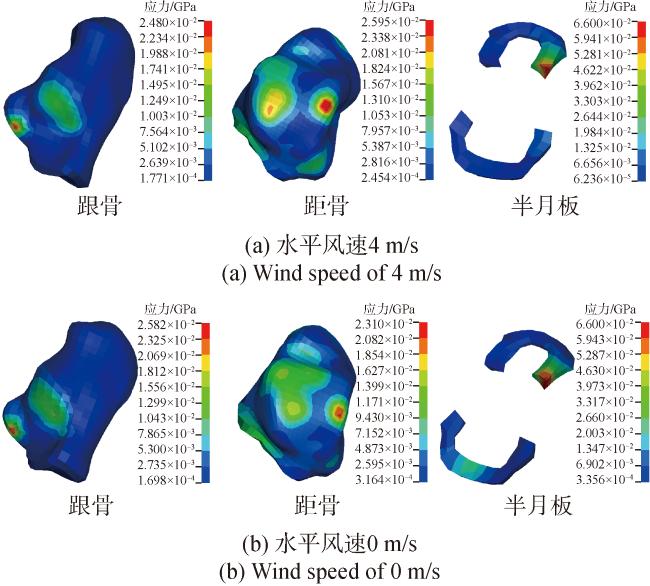
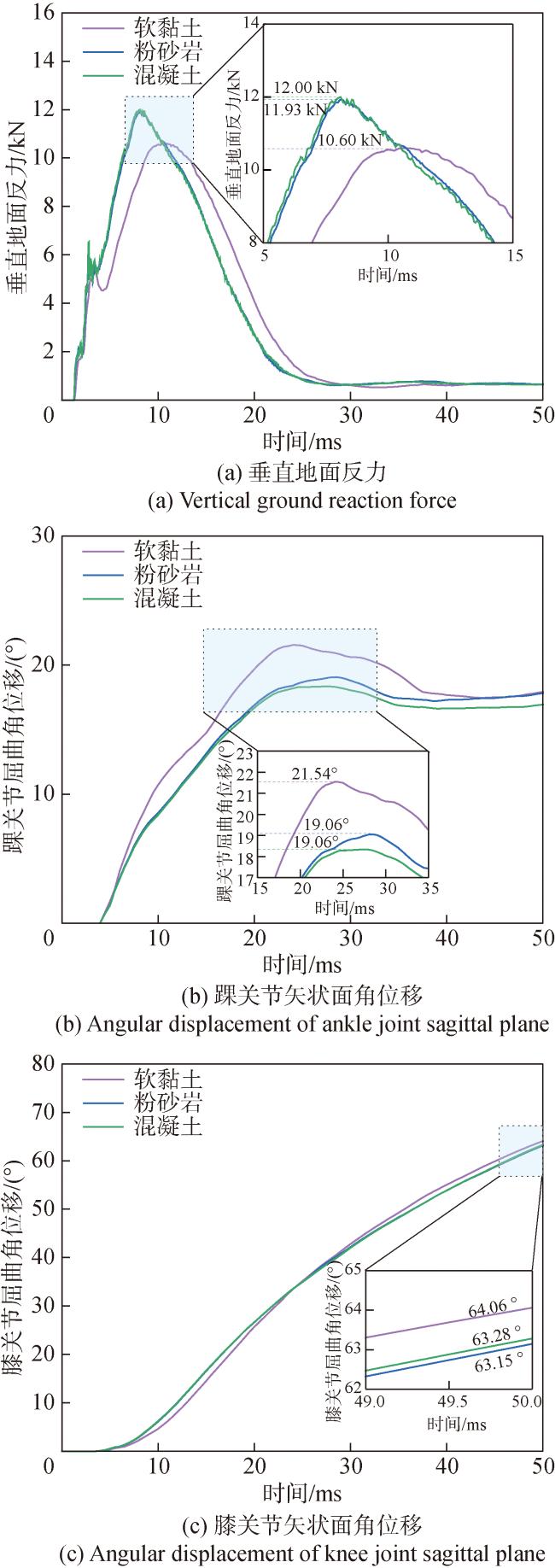
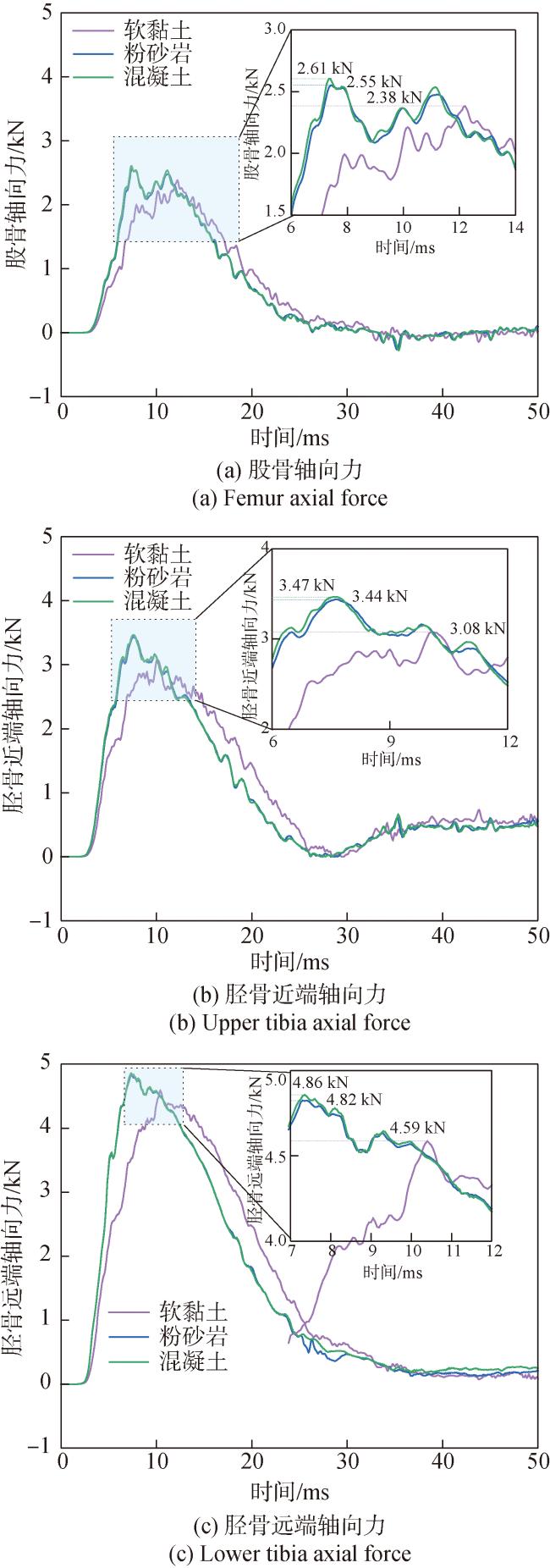
Fig.1 GHBMC full-body finite element modelFig.2 Posture adjustment of human finite element modelFig.3 Human landing impact finite element model Table 1 General information of subjectsFig.4 Location of reflective marker pointsTable 2 Comparison of platform landing experiemnts and simulationsFig.5 Comparison of experimental and simulated GRFs at different platform heightsFig.6 Comparison of experimental and simulated knee joint motion angles at different platform heightsFig.7 Comparison of experimental and simulated ankle joint motion angles at different platform heightsTable 3 Simulation parameter settings for analysis of descent speed effectTable 4 Simulation parameter settings for analysis of horizontal wind speed effectTable 5 Simulation parameter settings for analysis of ground condition effectTable 6 Injury criteria for lower limbFig.8 Data extraction locations for three injury assessment criteriaFig.9 Comparison of kinematic data at different descent speeds during landingFig.10 Comparison of lower limb injury indices during landing at different descent speedsFig.11 Comparison of peak stress in calcaneus,talus,and meniscus at different descent speedsFig.12 Comparison of kinematic data at different wind speeds during landingFig.13 Displacement of human center of mass at different wind speedsFig.14 Comparison of lower limb injury indices during landing at different wind speedsFig.15 Comparison of peak stresses in calcaneus,talus, and meniscus at different wind speedsFig.16 Comparison of kinematic data at different ground conditions during landingFig.17 Comparison of lower limb injury indices during landing at different ground conditionsFig.18 Comparison of peak stresses in calcaneus,talus, and meniscus at different ground conditions
Table 1 General information of subjectsFig.4 Location of reflective marker pointsTable 2 Comparison of platform landing experiemnts and simulationsFig.5 Comparison of experimental and simulated GRFs at different platform heightsFig.6 Comparison of experimental and simulated knee joint motion angles at different platform heightsFig.7 Comparison of experimental and simulated ankle joint motion angles at different platform heightsTable 3 Simulation parameter settings for analysis of descent speed effectTable 4 Simulation parameter settings for analysis of horizontal wind speed effectTable 5 Simulation parameter settings for analysis of ground condition effectTable 6 Injury criteria for lower limbFig.8 Data extraction locations for three injury assessment criteriaFig.9 Comparison of kinematic data at different descent speeds during landingFig.10 Comparison of lower limb injury indices during landing at different descent speedsFig.11 Comparison of peak stress in calcaneus,talus,and meniscus at different descent speedsFig.12 Comparison of kinematic data at different wind speeds during landingFig.13 Displacement of human center of mass at different wind speedsFig.14 Comparison of lower limb injury indices during landing at different wind speedsFig.15 Comparison of peak stresses in calcaneus,talus, and meniscus at different wind speedsFig.16 Comparison of kinematic data at different ground conditions during landingFig.17 Comparison of lower limb injury indices during landing at different ground conditionsFig.18 Comparison of peak stresses in calcaneus,talus, and meniscus at different ground conditions/
| 〈 |
|
〉 |



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}